Procedure
Breast Lift

Stretching of the breast skin due to past pregnancies, breast feeding, weight gain, genetics, or aging leads to loose skin and breast sagging / drooping (breast ptosis) as well as loss of upper breast fullness and contour and often enlarged nipple-areola complexes (NAC, the pigmented region around and including the nipples). Often, the NAC drops lower on the breast mound and may even point downward. The old method for deciding whether one needed a lift – holding a pencil underneath the breast – is definitely an indication of glandular ptosis (sagging); however, some patients might be happy with replacement of volume only without a “lift”. These patients may be more interested in volume than shape and placement of an implant or basically breast augmentation alone will be a good option for them. Other patients really desire upper breast fullness which can only be achieved with a lift. Although it may seem that filling up the skin envelope with a bigger implant will give upper chest fullness, it will not last. Ultimately, the patient will be bigger but also “ sag” or droop even more than before.
STAGING Breast Augmentation and LIFT Procedures
This is why Dr. Short may recommend staging. Basically she suggests doing the augmentation first, then deciding whether the lift is really desired. The patient may or may not want to trade additional incisions for a perkier look once they have more volume. This allows the patient to decide for themselves once the volume is replaced. Every patient has different ideals, so our goal at Gillian Plastic Surgery is to understand your goals and help you reach them.
If staging is not feasible, then we can help the patients decide by answering some questions.
- Did you like the way they looked when you were pregnant or breastfeeding?
- Are you happy with your size when you are wearing an uplifting but not padded bra? Or do you feel you want more volume ?
- Are you happy with the position and size of your areola?

The answers will help us determine together what approach will be the best for each individual patient. For example, if you are happy with your volume and you just don’t like what happens when you take off your bra, then a lift may be the perfect solution. If, however, in a nice un-padded push-up bra, you still want more volume along with that lift, then you likely want an implant in addition to your lift. We can help you visualize your results and make informed decisions.
Incisions For most, this is the biggest concern.
Dr. Short uses several incisions depending on the type of lift that is needed. If the entire breast volume / gland has dropped below the natural crease AND the NAC is also too low or pointing downward, then only a ”full lift” will restore upper breast fullness and a prettier shape. Dr. Short rarely uses the “anchor”type incision even for a full mastopexy. Her limited incision breast lift is performed with an incision around the nipple-areolar complex (pigmented region around the nipples) and extending vertical incision (like a lollipop).
If the breast gland is still at or above the crease and the NAC is low on the gland itself, it may be possible to do a “benelli” type lift limiting the incision to just around the NAC. The NAC can be decreased in size and lifted higher. This technique does not provide much breast gland lift, however. Finally, there are some patients who stretch more in the lower breast than the upper, so the NAC is rolled upward and is too high on the “sagging” gland. Dr. Short does a completely different lift procedure for this type of lift which involves an incision in the crease only.
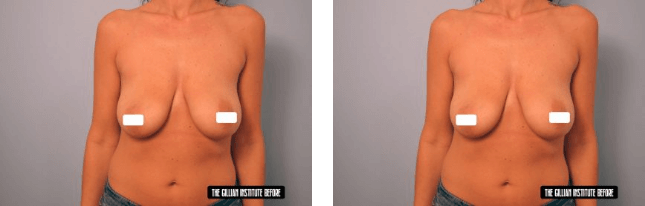
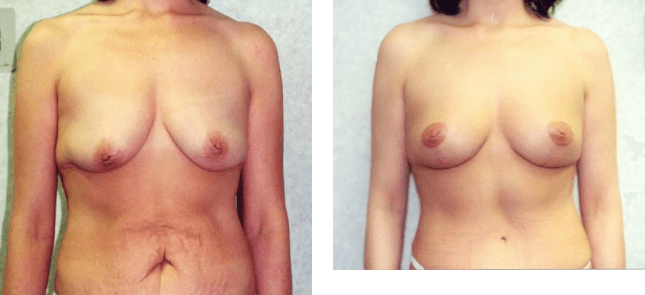
Mastopexy Alone
Some patients have adequate volume and really only need a lift. The patients pictured below both had a limited incision (lollipop) mastopexy.
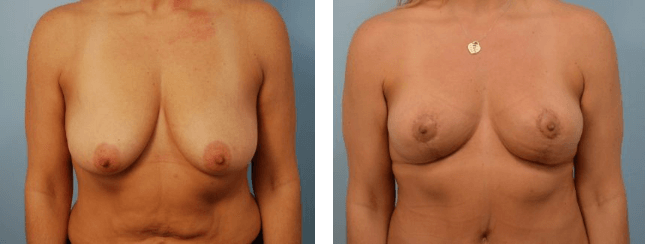
Mastopexy with Augmentation
If you have lost volume, have loose stretchy skin, and desire a better breast shape with increased volume you may need both tightening of the skin as well as an implant for the best result. This patient desired both tightening of the skin for a better shape as well as an increase in size.
Dr. Short uses several incisions depending on the type of lift that is needed. If the entire breast volume / gland has dropped below the natural crease AND the NAC is also too low or pointing downward, then only a ”full lift” will restore upper breast fullness and a prettier shape. Dr. Short rarely uses the “anchor”type incision even for a full mastopexy. Her limited incision breast lift is performed with an incision around the nipple-areolar complex (pigmented region around the nipples) and extending vertical incision (like a lollipop).
Natural Asymmetry Is Common
Due to the pre-existing asymmetry seen in the patient below, Dr. Short suggested she stage her procedures to obtain the best possible results. This patient had a mastopexy on the left and a breast reduction on the right followed by a staged breast augmentation to both sides. For longevity and maintenance of the symmetry, it is often better to make both breasts the same size and then augment them similarly rather than try to make the smaller one bigger to match the larger one.